While administering medications to people who are allergic is much less common than it used to be, these medical errors still occur with some frequency. This week’s case highlights a terrible case of a care provider’s failure to recognize a medication allergy, resulting in severe permanent damages.
What Happened
The patient was a young woman who had no major comorbidities. She went to a local emergency department with abdominal pain and was diagnosed with acute appendicitis. This particular hospital did not have a general surgeon on-call, so she was transferred to a neighboring facility for surgery.
The patient was given pain medication at the original facility and the transfer happened quickly and appropriately. The surgery went well with no major complications.
In the immediate post-operative period, the patient was nauseated and the nurse administered an anti-emetic medication (which was on the standard post-op order set).
Within minutes of medication administration, the patient had difficulty breathing, hypotension, and tachycardia. The staff did not immediately associate the change in condition with the medication, but rather assumed she was having internal bleeding or some other surgery-related complication.
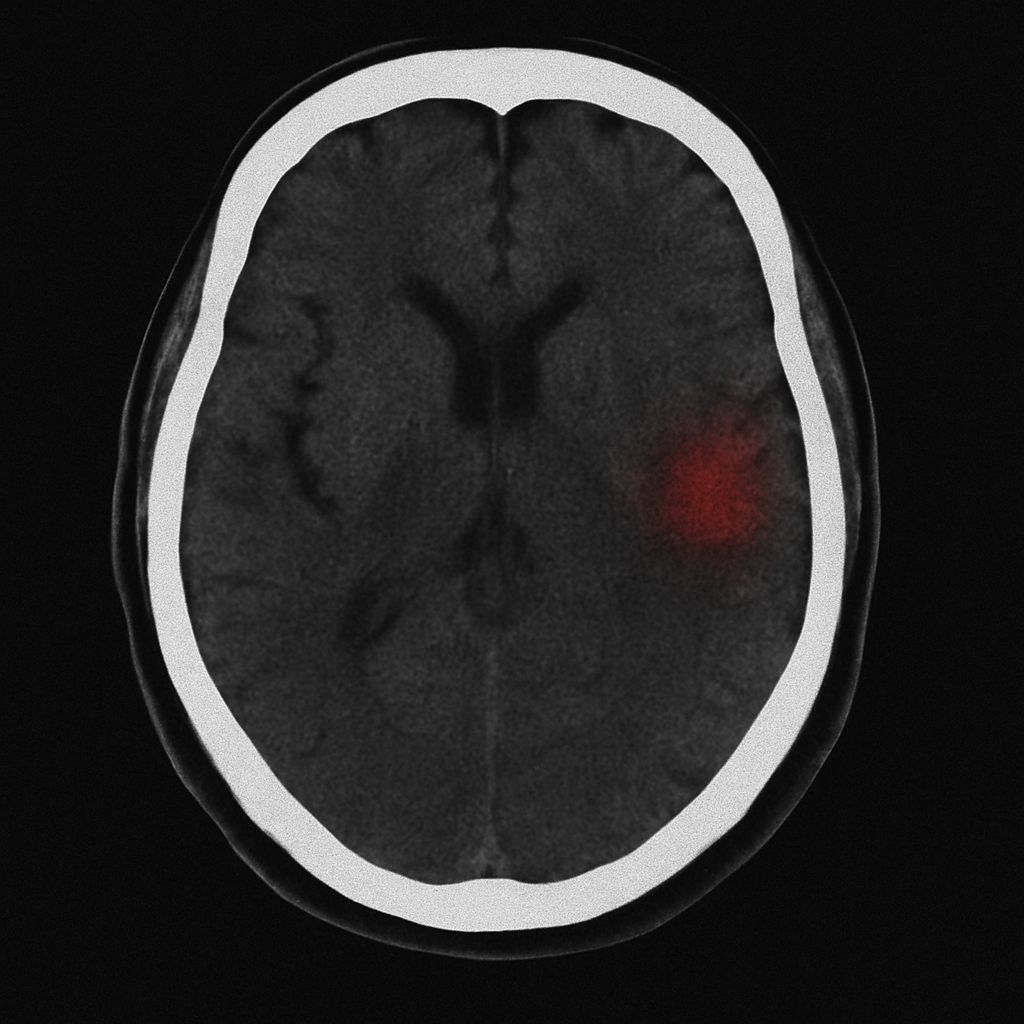
Eventually, the care team made the connection and treated the patient for anaphylaxis. Unfortunately, the delay in treatment resulted in intubation, a prolonged ICU admission, and subtle (but permanent) hypoxic brain injury.
What Went Wrong
It had been about two years since the patient had been cared for by the health system where the surgery took place. Between the time when she was last seen there and the date of the surgery, she had developed an allergy to the offending anti-emetic medication. The hospital where she was seen originally and diagnosed with appendicitis had correctly identified and documented this allergy in their records.
Unfortunately, when the patient was transferred for surgery, she was taken quickly to surgery and the records from the transferring facility were not thoroughly reviewed. Additionally, the patient received very strong pain medication just before transfer. She had already told the first facility about the allergy, so when asked by the staff at the second hospital whether she had any “changes in her allergies”, she responded “No”… because she’d already told the other care team about her anti-emetic medication allergy.
This miscommunication led to administration of a medication to which the patient had a known allergy, resulting in severe permanent damages.
How We See It
There is clear liability for the health system, but determining exactly who breached the standard of care presents an interesting challenge.
The transferring facility documented the patient’s allergy, but the transferring physician’s note was not completed and signed prior to transfer. Receiving physicians typically rely on transferring physicians’ records to make clinical decisions. That said, the nursing notes clearly identified the new allergy and this information WAS shared with the receiving facility.
Ultimately, we determined two different people breached the standard of care: the surgeon who ordered the medication and the nurse who administered it.
The surgeon did not complete an adequate history and relied on documentation from two years prior to determined allergies. The nurse in the recovery unit administered the medication without first asking about medication allergies (yes, the patient was awake, coherent, and would have recognized the name of this medication).
Causation and damages were fairly straightforward as the medical records clearly document the etiology of her clinical decompensation as an anaphylactic reaction to the anti-emetic medication.
Pre-Litigation Pearls
Allergy lists are one of those elements in the electronic health records that auto-populate into both nursing and physician notes. This give the impression that the care team asked about and properly documented medication allergies.
If you look more closely, though, you will USUALLY see date stamps for when these allergies were confirmed. Depending on when the notes were signed (or refreshed), it can be confusing to determine “who knew what and when” by just looking at a single note in isolation.
One trick our pre-litigation experts find useful is to look for the allergies in multiple locations throughout the medical records. We focus on allergy documentation from PRIOR visits, the CURRENT visit, and FUTURE visits. We also review the allergies documented by different physicians and nurses throughout the hospital admission in question. When we bring all this data together, it generally creates a clear picture of “who knew what and when”.
This level of detail is not necessary for every pre-litigation review, but it is absolutely critical when determining breach of standard and causation for medication allergy cases.
Submit a Case
Do you have a case on your desk and aren’t sure if it’s worth pursuing? Before you retain an expert, let our pre-litigation physician reviewers do an in-depth analysis and help you determine next steps. CLICK HERE to create an account and submit your case today.
(Cases in this series are real cases reviewed by our pre-litigation physician reviewers. We modify some details of the case and will occasionally modify some bigger factors to be certain the cases remain anonymous and can’t be identified by third parties. The take-home-points remain valid.)