Complications related to untreated high blood pressure are a very common reason people seek out an attorney for potential medical malpractice. The general public understands “High blood pressure is bad”… but there is much more nuance when it comes to the medical-legal implications of blood pressure management. Do you need an expert witness to review, or can you handle this on yourself?
What is hypertension?
Hypertension is just a fancy medical term for higher than “normal” blood pressure. More technically, hypertension is defined as a persistent elevation of blood pressure >130/80. SEVERE hypertension is when you start reaching blood pressures >180/110-120. Anything below this level is USUALLY not something that would cause an ACUTE problem for a patient. Long term, sure. But an acute problem like a brain bleed or aortic dissection… not likely. When an expert witness is making a merit determination, there is a lot to consider.
How do doctors address hypertension?
This depends very much on the clinical setting. In general, the MAJORITY of potential medical malpractice cases involve the management of acutely elevated blood pressure in the emergency department. Of course, there are some cases that originate in the primary care setting, but these are less common.
When an ED provider encounters a patient with severe hypertension (>180/110-120), they should first confirm the value is real and not a measurement error (this happens much more often than you might think). If the measurement is accurate and the reason for the ED visit is unrelated to the blood pressure, it is ALMOST always fine to proceed with the evaluation as if the blood pressure were not elevated, but recheck it a few times to be sure it comes down to a more normal, acceptable range. MANY people have pain and anxiety causing their elevated blood pressure, and some good old-fashioned relaxation is often all that’s needed.
HOWEVER, should the blood pressure remain elevated, or if the patient’s presentation is at all related to their elevated blood pressure, the physician must distinguish between HYPERTENSIVE EMERGENCY and ASYMPTOMATIC MARKEDLY ELEVATED BLOOD PRESSURE (formerly called Hypertensive Urgency).
Hypertensive Emergency
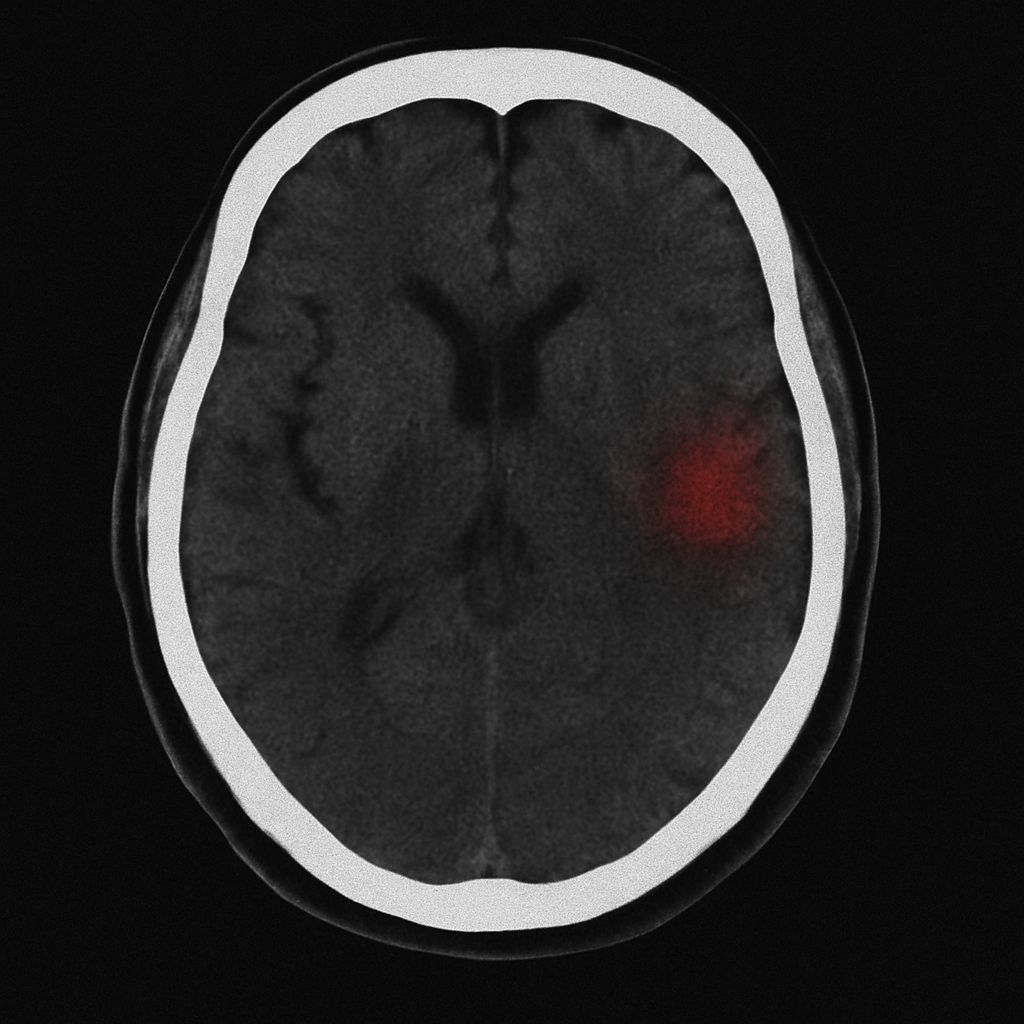
Hypertensive Emergency is defined as severe hypertension accompanied by evidence of new or worsening target-organ damage, such as acute injury to the brain (e.g., encephalopathy, stroke), heart (e.g., myocardial infarction, acute heart failure), aorta (e.g., dissection), kidneys (e.g., acute renal failure), or retina (e.g., papilledema).
Asymptomatic Markedly Elevated Blood Pressure
Asymptomatic Markedly Elevated Blood Pressure is simply as it sounds… severe hypertension without any symptoms or evidence of target-organ damage.
Why does it matter?
Physicians must distinguish between these two entities because it directly affects patient management. The work-up to make this distinction is beyond the scope of this post, but just recognize it takes labs, imaging, EKGs, etc.
Hypertensive emergencies require acute lowering of blood pressure (but not too fast or too low) to prevent further target-organ dysfunction.
Elevated blood pressures without target-organ damage should NOT have acute lowering of blood pressure, but CAN be started on long-acting antihypertensive medication with close follow-up 1-7 days. In the proper setting, and with VERY GOOD near-term follow-up, a physician is NOT necessarily required to initiate blood pressure medications, as these are best managed long-term by a primary care provider.
What do we see?
Our pre-litigation physicians frequently review cases where our attorney’s clients were upset their family member had a blood pressure “through the roof”, and it was not treated. More often than not, the blood pressure readings are well below the threshold for severe hypertension, meaning the case doesn’t have merit (well… at least not for the blood pressure reason… we find all kinds of other interesting facts along the way).
HOWEVER, our expert witness team does see a fair number of cases with severe hypertension that are not even remotely worked-up to the degree required to rule-out hypertensive emergency. We frequently see providers who simply give oral medication (usually Clonidine) to temporarily drop the blood pressure, get a “better number”, and discharge the patient before the severe hypertension returns. Sure, this makes clinicians feel better, but it does nothing for the patient and is not the standard of care for management of severe hypertension.
What should you do as an attorney?
When you review records and the patient/family are concerned about untreated high blood pressure… you should… well… look at the blood pressures. If they are <180/110-120… the likelihood you have a case is much lower. If the pressure is higher than that range, it could be medical malpractice, and it’s probably worth it to get a review… either from our pre-litigation team or a testifying expert on our platform.
CLICK HERE if you have a case for our pre-litigation physician team. We can get it reviewed and back to you with our recommendations in less than a week.