Failure to diagnose stroke is one of the most common cases our attorneys bring to us for pre-litigation analysis. The vast majority of these cases end up with an affirmation of breach in standard of care, but a “DO NOT PURSUE” recommendation based on causation. This post will go through the most simple but effective way to evaluate stroke cases in the medical-legal context.
What is a stroke?
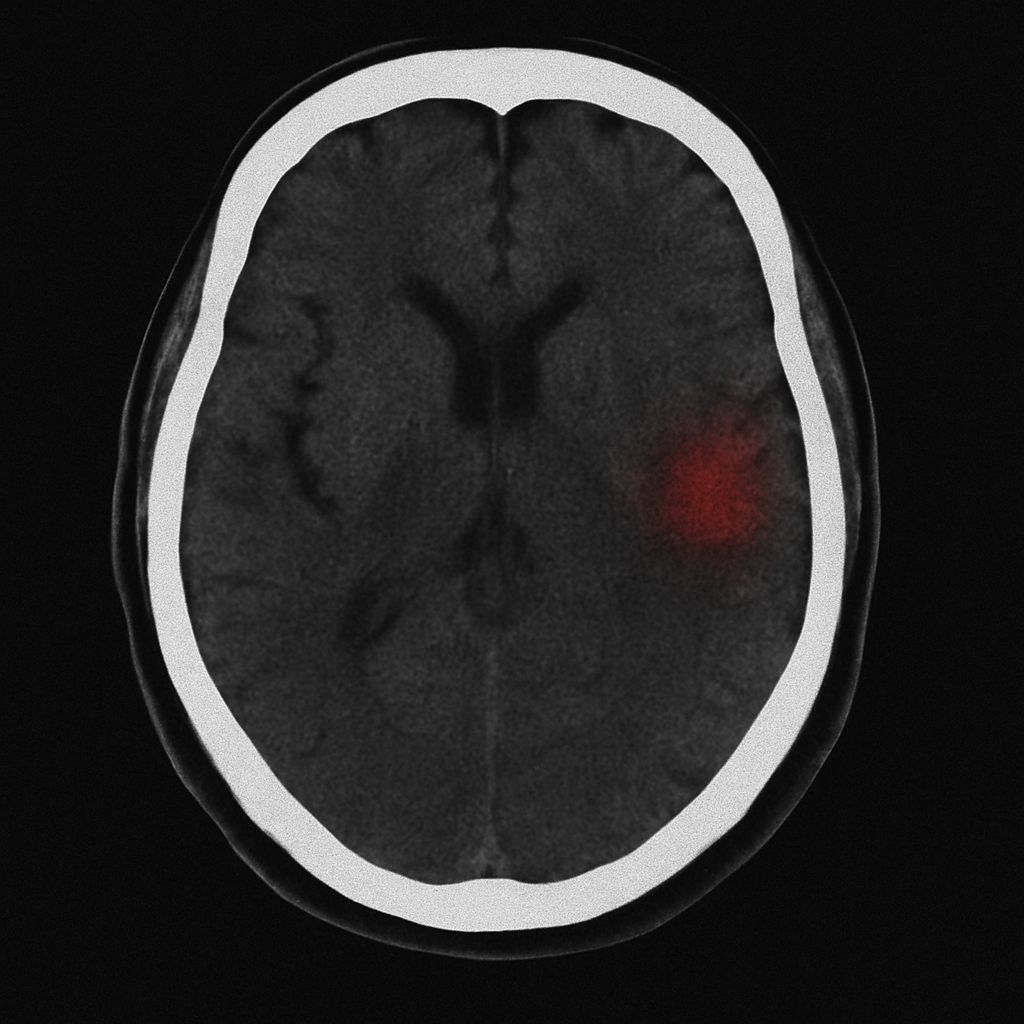
For the purpose of this post, we will be primarily focused on ISCHEMIC STROKE. This is a stroke caused by a blood clock blocking an artery in the brain. Patients can also have hemorrhagic stroke (bleeding in the brain), but the management of these types of strokes is very different and warrants its own post.
How do you treat an ischemic stroke?
While there are measures you can take to mitigate the effect of stroke and prevent secondary stroke, the primary question in malpractice case typically involves whether the failure to diagnose a stroke prevented the administration of THROMBOLYTIC medication to “dissolve the clot”. The primary thrombolytic medication used for this purpose is alteplase , although tenectaplase is now widely used by many facilities. The science behind this is beyond the scope of this post, so we will just use the term “thrombolytic” to avoid confusion. This medication is delivered through an IV must be administered within a very narrow window of time to be effective and safe.
In addition to IV administration of thrombolytics, stroke patients with LARGE VESSEL OCCLUSIONS can often be treated with an interventional procedure known as a thrombectomy. This is a very select group of patients with large strokes in large arteries of the brain. Despite the smaller set of patients for which this treatment can be effective, it has the benefit of a much wider time window (around 24 hours).
Who can safely get treatment for an acute stroke?
Here is where things get tricky. The INCLUSION and EXCLUSION criteria for thrombolytic treatment for acute ischemic stroke are very stringent. Patients must be diagnosed and treated within a very specific time window to safely receive thrombolytics. They must have fairly significant symptoms… but not too severe. Their blood pressure has to be within a reasonable range. They can’t be on certain medications. They can’t have had any recent surgeries…. and… well… there are LOTS of criteria.
So if you are an attorney reviewing your own records and want the quick and dirty approach… here are the major things you need to look for:
- LAST KNOWN WELL (LKW) – When was the last time the patient was seen behaving normally and not exhibiting ANY stroke symptoms? If it was longer than 4.5 hours, they probably weren’t eligible for thrombolytics… UNLESS they have a large vessel occlusion (LVO)… in which case they could have up to 24 hours to safely get a thrombectomy.
- NIHSS – This is a standardized score based on a very specific physical exam procedure. It provides a fairly objective, measurable degree of stroke severity. If the score is really low (<5), the risk/benefit of thrombolytics might not be worth it. If it is crazy high (>25), the risk might also be too high. HOWEVER… even very low NIHSS scores can still be permanently disabling, so you can’t rely solely on the score. Yeah… it gets tricky.
- MEDICATIONS – Some “blood thinners” make thrombolytics unsafe. Warfarin, for example, is an absolute contraindication to giving thrombolytics (assuming the INR is >1.7). Plavix, on the other hand, is a RELATIVE contraindication, meaning you CAN give thrombolytics, but you need to think about it and weight the extra risk.
There are MANY other factors to consider, but this will get an attorney started. If you figure out these factors, you can make a reasonably good decision to keep the case moving through the process or turn it down.
“But I thought this post was about DIAGNOSING stroke?”
Here is the (unfortunate) reality… most strokes present to the hospital well outside the treatment window. For those that do present within the window, there are frequently contraindications to treatment with thrombolytics. So… even if the physicians miss the diagnosis, it USUALLY does not make any difference to outcome. Yes, there are medications and interventions that can prevent future stroke and accelerate recovery, but these are typically minor points and very difficult to objectively measure. So… the lack of diagnosis typically only matters if it prevented treatment with thrombolytics.
In reality, physicians are very good at identifying treatable strokes. Sure, they still miss subtle strokes and can misdiagnose patients… but it’s pretty rare.
So should you even consider these cases for litigation?
Yes… absolutely! Even with all the challenges of time windows, contraindications, etc… there are MANY more factors to consider.
- Posterior circulation strokes are still FREQUENTLY misdiagnosed and have a potentially longer treatment window.
- Strokes occurring in hospitalized patients frequently go unrecognized… making the time window less of an issue.
- Many of the contraindications to treatment are RELATIVE and not ABSOLUTE
- Failure to take an adequate history frequently leads to an incorrect determination of Last Known Well
- etc…
Where do you go from here?
The next time a stroke case comes through intake, simply recognize the most important data points to discover: Last Known Well, NIHSS, and Medications. This information will get you 75% of the way there. If you can check those boxes, it’s worth it to get a pre-litigation consult from one of our physician experts. Otherwise, it’s PROBABLY not a case worth pursuing… but not definitely.
OK…I confess… it is complicated… but stroke cases are really some of the most straightforward cases we review. We are here to help if you need us.
Have a case?
If you need our pre-litigation team to review your case… or if you need a testifying expert… CLICK HERE and we will take it from there.